Peds ID Abx QOTW #6 Answer
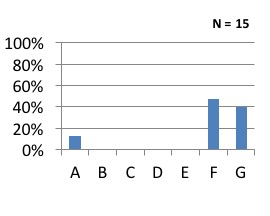
f) Treat with Amox/Clav for 10 days
This is how others answered:
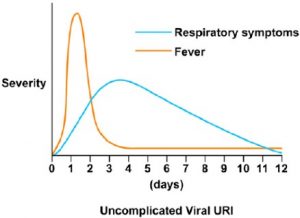
Viral URI Typical Progression
- Viral URI with fevers, myalgias, headaches in first 2-3 days
- Secretions begin clear (1-2days), become mucopurulent (3-5 days), then again clear or dry up prior to resolving completely
- Most resolve by ~10 days but not all
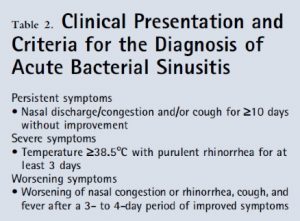
Acute Sinusitis
- Symptoms show no improvement at >10 days
- Less than 30 days (acute)
- Others symptoms include:
- Persistent secretions or worsening of secretions with fevers
- Malodorous breath
- Tooth or facial pain
- Persistent fevers
- Persistent cough day and night time
- Sudden worsening of URI symptoms
 Pediatr Rev. 2013 Oct;34(10):429-37
Pediatr Rev. 2013 Oct;34(10):429-37
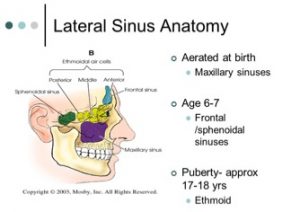
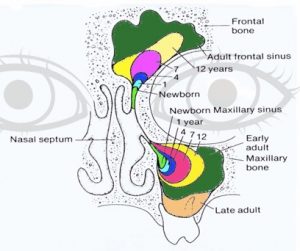
Sinus Development in Children
- Sinus development in children should be considered in the diagnosis of sinusitis
Imaging in Diagnosis of Acute Sinusitis
- CT/MRI scans are the most useful test for imaging sinuses, although diagnosis is usually made clinically
- Findings include complete sinus opacification, mucosal thickening of at least 4 mm, or an air-fluid level.
- Imaging in presence of viral URI shows abnormalities in ~80% of viral infections
- Negative imaging excludes the diagnosis, but a positive image does not make the diagnosis
- Plain films are considered insensitive and should not be done
Microbiology of Acute Sinusitis
- Mirrors the etiology of acute otitis media (AOM)
- S. pneumoniae, H. influenzae, M. catarrhalis are the typical pathogens
- S. aureus is not a common pathogen and should not be routinely consider outside of complications from sinusitis
- Aspiration of sinuses or other testing of nasopharynx is not warranted based on available data (e.g. nasopharyngeal swabs or cultures from nares)
- Treatment failures should be referred to otolaryngology for evaluation for possible aspiration
Treatment of Acute Sinusitis
- Options for therapy include (typically 10 days for children, but short courses of 5 days for adolescents may be effective)
- Amoxicillin alone (but increasing rates of H. influenzae resistance)
- Can be considered, but probably second line
- Amoxicillin/clavulanate (45mg/kg/day divided BID)
- Preferred therapy
- Cefidinir (14mg/kg/day qday or BID)
- Second line
- Cefuroxime (30mg/kg/day divided BID)
- Second line
- Levofloxacin (16mg/kg/day divided qday or BID based on age)
- Should be reserved for cases in which no other options exist
