Peds ID Abx QOTW #3 Answer
The correct answers are:
a) Do nothing and treat symptomatically
b) Perform rapid Influenza, if positive treat with Tamiflu
c) This is possibly strep pharyngitis, do a rapid Strep test and treat if positive
d) Centor Criteria suggest high probability, no need to test, treat for strep
e) Send Serology for EBV
f) Send a Monospot
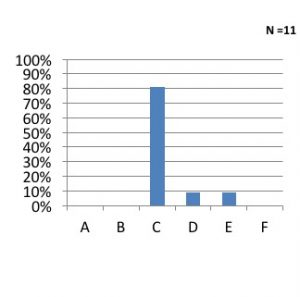
Here’s how other respondents answered:
ID Attending Discussion:
Deciding when to treat for Group A Strep
- Clinician Prediction
– PPV 29%
– NPV 78%
- Centor Criteria
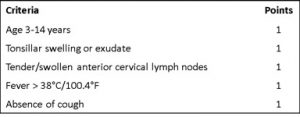
– Area under the ROC = 70% (fair)
– Leads to over treatment
- If anyone has symptoms, including exudative tonsillitis alone, a test should be done to determine who needs treatment
Recommended Testing
- School aged children with suspicion for GAS should have a rapid test done
– If positive rapid strep, treat
– Backup culture should be sent for children who have a negative test
– Treatment of high risk patients with negative rapid test while pending culture can be considered
- Who is at highest risk = higher Centor Criteria
- Consider alternative diagnosis
– EBV in teenager with exudative tonsillitis
- Rash with PCN for treatment of GAS + exudative tonsillitis, consider testing for EBV as well
Treatment recommendations for GAS
- Adults and adolescents
– PCN VK 500mg PO BID x 10 days (narrowest spectrum)
– Cephalexin 500mg PO BID x 10 days (PCN allergy with Rash)
– Azithromycin 500mg qday x 5 days (Severe PCN allergy)
- Children
– Amoxicillin 50mg/kg (max 1gm) po qday x 10 days
– Cephalexin 20mg/kg (max 500mg) po BID x 10days (PCN allergy with Rash)
– Azithromycin 12mg/kg (max 500mg) x 5 days (Severe PCN allergy)
EBV Testing
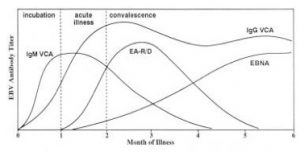
- At Harbor-UCLA, EBV serology is much faster than a Monospot (other institutions may vary)
– EBV serology Panel
- EBV VCA IgM Ab
- EBV VCA IgG Ab
- EBV EBNA Ab
– Monospot in most hospitals is faster
- Test for heterophile antibodies (not EBV specific)
- Higher PPV in adolescents, low PPV in younger children
– EBV PCR should not be done
- Large % of patients will have low grade viremia without disease
