Peds ID Abx QOTW #4 Answer
The appropriate first-line antimicrobial therapy is:
c) Amoxicillin low dose for 10 days
d) Amoxicillin high dose for 10 days
Here’s how others answered:
Treatment Guidelines
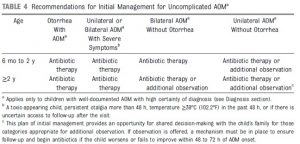
Pediatrics 2013;131:e964–e999
Patient Management Recommendations
- Options for this patient include
1) Start antimicrobial therapy
2) Observation of the patient
3) Observation with a “Wait and see” Rx (aka Safety Net Antibiotic [SNAP] or Delayed Rx)
- What is the best option? Probably a wait and see approach would be best
“Wait and See” or Delayed Rx
- Study in 2003 found that patients given pain management and Delayed Rx filled them only 31% of the time (Pediatrics 2003;112:527–531)
– Parents whose child had had more than 2 AOM treated with antimicrobials more likely to fill
- For parents who are really concerned, giving them an Rx to be filled in 48hrs if not improved may provide a reassuring way to decrease antibiotic use
Antibiotic Choice in AOM

Why Amoxicillin over others?
- While the most common cause is viral, the second most common is S. pneumoniae
– Rates of resistance to PCN are on the decline after PCV13 introduction
- Drug of choice remains amoxicillin up front, for S. pneumoniae coverage
– Dosing somewhat controversial
- High dose 80-90mg/kg is recommended
- Data for this recommendation debatable and experts in the matter argue that low dose amoxicillin (40-45mg/kg) has similar failure rates
- Augmentin as second-line for beta-lactamase producing Haemophilus spp. and Moraxella spp.
- Cephalosporins maintain activity in beta-lactamase producing strains of Haemophilus and Moraxella, and have higher activity against PCN resistant S. pneumoniae
